By Sabrina Corlette
The Inexpensive Care Act (ACA) Marketplaces simply skilled one other record-breaking enrollment season, with over 21 million folks deciding on a Market well being plan for 2024. The Facilities for Medicare & Medicaid Companies (CMS) is rightly celebrating that accomplishment whereas working to construct on the progress and enhance the patron expertise. In November, CMS and the Treasury Division proposed a brand new set of requirements and necessities for the Marketplaces and well being insurers for plan 12 months 2025 via the annual “Discover of Profit & Fee Parameters” (NBPP). The ultimate rule is anticipated quickly.
The proposed 2025 NBPP acquired over 200 stakeholder feedback through the public remark interval. CHIR reviewed a pattern of feedback from three main stakeholder teams to higher perceive the potential impression of the proposed guidelines. This primary weblog in our three-part collection summarizes feedback from medical insurance corporations, their consultant associations, and brokers. The following two weblog posts will summarize feedback from client advocacy teams and state departments of insurance coverage and state-based Marketplaces (SBM). For this publish, we reviewed feedback submitted by:
America’s Well being Insurance coverage Plans (AHIP)
Affiliation of Neighborhood Affiliated Plans (ACAP)
Blue Cross Blue Defend Affiliation (BCBSA)
CVS Well being (previously Aetna)
The proposed 2025 NBPP covers a variety of points (an in depth abstract of its provisions, in two components, is on the market on Well being Affairs Forefront right here and right here). This abstract of insurance coverage firm and dealer suggestions focuses on chosen CMS proposals: (1) The method and requirements for states to transition and preserve an SBM; (2) updates to the important well being profit (EHB) requirements*; (3) particular enrollment intervals (SEP) for low-income people; (4) insurance policies for people who fail to reconcile their premium tax credit at tax time; and (5) limits on non-standardized well being plans.
New SBM Processes and Requirements
By 2026, 20 states and the District of Columbia are anticipated to function their very own SBM, with Georgia and Illinois quickly becoming a member of the present 19. Extra states, comparable to Michigan and Arizona, are contemplating laws to run their very own SBMs. On this proposed rule, CMS would set new expectations for states endeavor this transition, and new national-level requirements for Market plans and operations.
Course of for changing into an SBM
Normally, the insurers and brokers that commented on proposed course of adjustments, such because the requirement that transitioning states first spend a 12 months as an SBM on the federal platform, have been supportive. BCBSA and Cigna noticed that such a staged transition would give states satisfactory time to implement essential infrastructure adjustments. HealthSherpa urged CMS to require that transitioning states doc how they might make up for enrollment losses, if they do not want to make use of the Enhanced Direct Enrollment (EDE) performance that now drives a lot of HealthCare.gov’s enrollment.
Community Requirements
Medical health insurance corporations have been much less welcoming of proposals to lift the bar for Market plans by extending the federal Market’s community adequacy requirements to insurers taking part in SBMs. Of the feedback reviewed, solely Cigna expressed any help for establishing a nationwide ground for community adequacy throughout Market platforms. The corporate applauded the trouble to have “extra constant and uniform necessities” for multi-state issuers. Nonetheless, Cigna requested that CMS present an extra 12 months to implement the coverage by suspending the efficient date to January 1, 2026.
The opposite insurers and associations in our pattern strongly opposed extending federal time and distance requirements, arguing that state insurance coverage regulators are greatest positioned to set these requirements. “States have specialised information of native geography, care patterns, and market dynamics,” AHIP commented. The commerce affiliation additional noticed that many states apply their community adequacy requirements to all the industrial market, and having a separate set of federal requirements for Market plans would “bifurcate” the market and create administrative complications. BCBSA had comparable considerations, noting {that a} “one-size-fits-all” method would reduce insurers’ skill to “differentiate” their networks, making it tougher to supply a decrease price possibility for shoppers.
Standardized plans
Well being insurers equally opposed the concept of extending plans with standardized profit designs to SBMs. Right here once more, insurers argued that states are “in the most effective place” to find out whether or not standardized plans are acceptable for his or her residents (AHIP). BCBSA additional urged that SBMs be allowed to determine “progressive” insurance policies that meet the wants of their markets.
Internet brokers and Direct Enrollment/Enhanced Direct Enrollment Entities
Noting that there’s “elevated curiosity” amongst SBMs in using internet brokers or direct enrollment (DE)/EDE entities to help with eligibility and enrollment features, CMS would lengthen federal Market requirements for these entities to all Marketplaces. Well being insurers and brokers have been largely supportive of those proposed adjustments, with a number of exceptions.
ACAP applauded the proposal, noting that web-brokers are sometimes headquartered outdoors of the states through which they’re aiding shoppers, suggesting a necessity for a nationwide set of protections. “Standardization is a robust software to forestall abuses,” the affiliation famous. ACAP additionally requested CMS to do extra to cut back client confusion with DE/EDE entities that market non-Market merchandise, comparable to short-term restricted period insurance coverage.
Conversely, BCBSA objected to the proposal, urging as an alternative stronger CMS oversight of brokers and brokers. BCBSA identified that, for the plan 12 months 2023 open enrollment interval, the federal Market had “massive will increase in unauthorized enrollments.” BCBSA noticed that in lots of circumstances these fraudulent enrollments, typically executed with no client’s information or consent, have been pushed by internet brokers who have been out-of-state.
HealthSherpa and eHealth each usually supported the online dealer and DE/EDE proposals. eHealth famous that uniform requirements for internet brokers and DE entities assist “guarantee a degree enjoying discipline and oversight to make sure enrollees are handled equally.” In addition they steered that constant requirements would give shoppers extra confidence in these entities as trusted sources of eligibility and enrollment assist. HealthSherpa additionally supported new necessities that might assist stop shoppers from inadvertently enrolling in non-Market plans.
HealthSherpa and eHealth additional noticed that internet brokers and DE/EDE entities now drive a lot of HealthCare.gov enrollment. In 2022, these channels accounted for 57 p.c of enrollment, and sure contributed to the numerous features of the 2024 enrollment season. To raised illuminate this impression, eHealth urged CMS to publicly launch plan choice and enrollment information for EDE and DE channels on a extra common foundation.
Updates to Important Well being Profit (EHB) Requirements
The ACA requires states to bear the prices of any state profit mandates which can be enacted after December 31, 2011 which can be along with the EHB. On the identical time, states can choose a brand new or revised EHB-benchmark plan with out going through an obligation to defray the price of extra advantages as long as the plan meets sure requirements. CMS has acquired suggestions from states that they’ve struggled to operationalize the “defrayal” coverage, and that some state efforts to mandate sure advantages may unintentionally be eradicating EHB protections from advantages already included within the state’s EHB-benchmark plan. States have additionally expressed concern in regards to the requirements underneath which they’re able to change their EHB-benchmark plan. Guidelines promulgated for 2019 require states to satisfy two scope of profit requirements:
- The typicality commonplace. The plan should present advantages equal to these supplied underneath a typical employer plan.
- The generosity commonplace. The plan should present advantages that don’t exceed the generosity of essentially the most beneficiant plan amongst a set of comparability plans.
On this draft rule, CMS proposed changes to the EHB defrayal coverage and the requirements adopted in 2019 that govern updates to the EHB-benchmark plan. As well as, the company proposed adjustments to how prescribed drugs are lined within the EHB.*
Defrayal and EHB replace adjustments
Well being insurer feedback in our pattern unanimously opposed the proposal to permit state profit mandates that, if already lined by the EHB benchmark plan, wouldn’t set off a defrayal obligation. In addition they beneficial in opposition to finalizing the proposal to remove the generosity take a look at when assessing states’ proposed adjustments to their EHB benchmark plans. Insurers argued that each adjustments would end in premium will increase. AHIP and BCBSA additionally decried the proposals as regulatory overreach inconsistent with the textual content of the ACA’s defrayal provision; AHIP argued that the adjustments would render the ACA’s “price defrayal obligation a nullity,” whereas BCBSA asserted that they have been “inconsistent with [c]ongressional intent.” CVS Well being additionally flagged that the proposals would create “vital monetary prices with no guardrails,” and an “unprecedented degree of annual volatility in EHBs.” The corporate lamented the impression on employers specifically, asserting that they are going to be confronted with the troublesome option to pay increased prices or take away some profit choices.
Pharmaceuticals in extra of EHB
CMS has proposed that if a plan covers prescribed drugs in extra of these lined by a state’s EHB benchmark plan, they might be thought-about EHB. This is able to require well being plans and insurers to rely the price of these medicine in the direction of enrollees’ annual most out-of-pocket prices and the ACA’s ban on annual and lifelong greenback limits on advantages. The well being insurers in our pattern usually opposed this proposal of their feedback. BCBSA urged CMS to additional examine the impression of such a coverage, noting that many third-party directors for employer-based plans use “copay maximizer applications” to seize affected person help {dollars} supplied by drug producers. BCBSA notes that underneath such applications, enrollees can entry medicine outdoors of EHB, typically with out cost-sharing. If CMS’ proposal is finalized, well being plans would wish to broaden the variety of medicine which can be thought-about EHB, making them ineligible for a copay maximizer program.
Figuring out what medicine to cowl: proposed change in U.S. Pharmacopeia methods
To fulfill EHB requirements, insurers should cowl at the very least the identical variety of medicine in each class and sophistication as outlined underneath the USA Pharmacopeia (USP) Medicare Mannequin Tips (MMG), or one drug in each class and sophistication—whichever is bigger. CMS has acquired stakeholder suggestions that the USP MMG has gaps in protection, significantly for weight problems, infertility, and sexual issues, and is up to date sometimes. Due to this fact, on this proposed rule the company sought feedback on whether or not to switch the USP MMG with the USP Drug Classification system (DC) to categorise the prescribed drugs required to be lined as EHB.
Well being insurers usually opposed switching to the USP DC system. Feedback famous that the extra granular USP DC system would require insurers to cowl medicine with, based on AHIP, “weak or poor proof” of scientific profit. Cigna supported switching to a brand new classification system, however the insurer argued that the USP DC may require protection of infertility medicine, sexual dysfunction medicine, and weight reduction medicine that at present fall outdoors the EHB. Ought to CMS transfer ahead with this proposal, Cigna urged the company to carve out these classes as “non-EHB.”
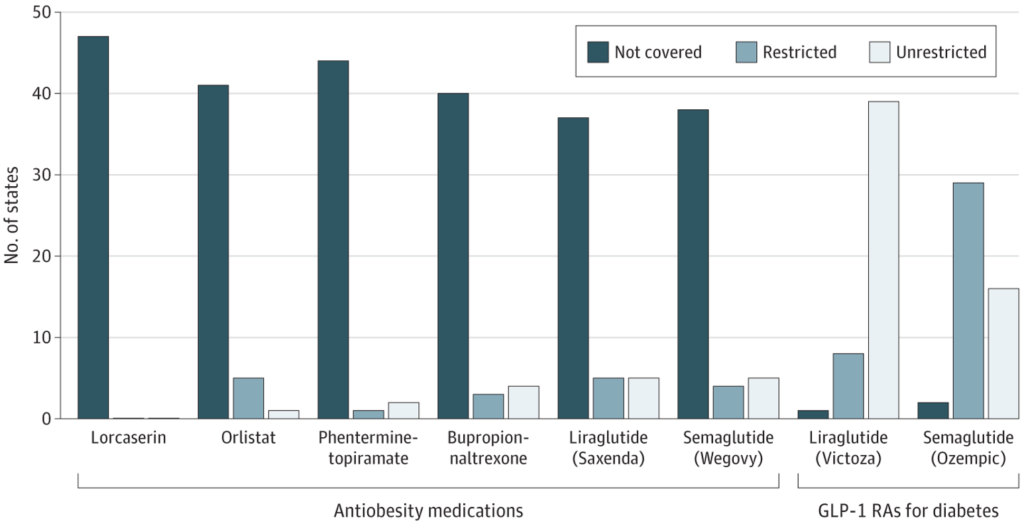
CMS additionally sought feedback on the protection of anti-obesity medicine, significantly the brand new GLP-1 class of medicines. The medical insurance corporations in our pattern have been uniformly against necessities to cowl GLP-1s. ACAP argued that the monetary prices of masking these medicine would “disproportionately drawback” small, native plans that serve areas with a excessive incidence of weight problems. BCBSA steered that mandates to cowl these medicine shouldn’t go into impact with out extra proof of their long-term scientific effectiveness and medical necessity.
Shopper illustration on P&T Committees
CMS has proposed to require, starting in plan 12 months 2026, that insurers’ Pharmacy & Therapeutics (P&T) Committees embody at the very least one client consultant. Well being insurers unanimously expressed reservations about this proposal, citing two main considerations: (1) client representatives would lack the required scientific and technical experience required to meaningfully take part on a P&T Committee, and (2) many so-called “client representatives” are in actual fact financially supported by the pharmaceutical trade. If the proposal strikes ahead, insurers argued that “sturdy battle of curiosity protections” and scientific experience ought to be required.
SEPs for Low-Revenue People
The 2022 NBPP created a month-to-month particular enrollment alternative for people at or under 150 p.c of the federal poverty degree (or $21,870 in annual earnings for a single particular person in 2023), however provided that the patron can enroll with a 0 p.c premium contribution after premium subsidies. In impact, this SEP is barely out there due to briefly enhanced premium tax credit licensed underneath the Inflation Discount Act (IRA). With these subsidies slated to run out on the finish of 2025, CMS is proposing to make this low-income SEP everlasting by lifting the requirement that enrollees have a 0 p.c premium contribution.
Well being insurers in our pattern opposed this coverage, arguing that making the low-income SEP everlasting would end in, as ACAP put it, “modified habits” that might immediate hostile choice and elevated premiums. AHIP predicted that this SEP, if finalized would end in “fixed enrollments and disenrollments,” and Cigna argued that this volatility, mixed with “the inadequacies of threat adjustment,” would deteriorate the danger pool and destabilize the Marketplaces.
Failure to Reconcile Advance Premium Tax Credit (APTCs)
CMS has proposed to require that Marketplaces give enrollees advance discover if they’re vulnerable to dropping premium tax credit score eligibility as a result of they didn’t file and reconcile these tax credit on their tax return. Marketplaces must notify enrollees of this threat after one 12 months of failing to reconcile premium tax credit (a 12 months upfront of dropping these premium tax credit). The insurers in our pattern have been largely supportive of this proposal. BCBSA, for instance, noticed that customers usually tend to keep enrolled if they’re notified earlier than they lose premium tax credit, quite than after the very fact, as a result of they nonetheless have a chance to replace their eligibility and retain monetary help.
Limits on Non-Standardized Plans
Presently, Market insurers on the HealthCare.gov platform can provide solely 4 non-standardized plan choices per service space in every of the next classes:
- Product community sort;
- Metallic degree (excluding catastrophic plans); and
- Inclusion of dental and/or imaginative and prescient protection.
This four-plan restrict will drop to 2 for every class for plan 12 months 2025 and past. Within the proposed 2025 NBPP, CMS would provide an exceptions course of to permit extra non-standardized plan choices for plans with decrease cost-sharing for providers that deal with continual or excessive price circumstances.
Well being insurers urged CMS to not transfer ahead with the two-plan restrict in 2025, arguing that doing so can be disruptive to enrollees and stifle innovation. AHIP additionally requested CMS to delay the two-plan restrict till they might consider and publish information on the impression of the present four-plan restrict, together with information on what number of shoppers enrolled or re-enrolled in standardized plan choices, what number of shoppers have been required to change to a brand new plan, client satisfaction scores, and agent and dealer suggestions on the plan limits. Oscar equally expressed concern in regards to the impression of the two-plan restrict, arguing that “crosswalking”—the method of enrolling a client in a brand new plan when their previous one is discontinued—is disruptive to members. The corporate argued that customers want selection in plan option to account for various well being wants and demographic components.
The carriers usually appreciated the proposed exceptions course of however discovered it too slim. For instance, whereas ACAP agreed with CMS considerations in regards to the threat of “alternative paralysis” for shoppers confronted with too many plans, they urged CMS to broaden the factors underneath which carriers may request an exception. A number of of the insurers in our pattern steered exceptions for plans primarily based on components comparable to totally different supplier networks or formularies, HSA eligibility, diminished cost-sharing for telehealth, or digital main care.
*Stakeholder feedback on one other CMS proposal to ease states’ skill so as to add grownup dental providers to the EHB benchmark plan, will likely be mentioned in a separate, forthcoming weblog publish.
A Notice on Our Methodology
This weblog is meant to supply a abstract of feedback submitted by insurance coverage corporations, consultant associations, and brokers. This isn’t supposed to be a complete assessment of all feedback on each provision within the proposed 2025 NBPP, nor does it seize each part of the reviewed feedback. To view extra stakeholder feedback, please go to https://www.rules.gov/.